

Two decades of experience in treating patients...

This is a narrow strip of synthetic material placed in your body to support the urethra. The 'Monarc subfascial hammock' is a brand name for such a tape made by a company called American Medical Systems (AMS). The hammock cradles your urethra and gives it a solid point to rest on and press against. This helps the urethra close more tightly at times of stress.
In women who have incontinence due to weakness in the pelvic floor and poor support of the urethra (i.e. "genuine stress incontinence"), 8 or 9 out of 10 women should be completely dry or much better after surgery than before. Nine out of every 10 women are able to be as active as they like after placement of a transobturator tape e.g. lift children, dance or exercise. As a result, 19 out of every 20 women are satisfied by the results of the procedure.
No-one can guarantee that everyone will be cured and about 1 in 20 women are not satisfied by the operation. If the bladder is overactive as well, then the success rate is less and fewer women are satisfied. In addition, side-effects are always possible and it is important to think carefully about the advantages, alternatives and risks of any procedure before going ahead.
In general, you will be dryer once the catheter is removed. The full improvement may take several weeks to be noticed.
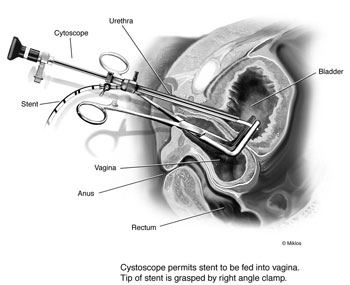
You have either a general anaesthetic so you are asleep or the lower half of the body is made to feel numb by a spinal anaesthetic. A small incision (about 1 to 1.5 inches, 3 cm) is made in the vagina just below the opening of the urethra (water pipe), and two 1/4 inch (0.5 cm) incisions in the inner thigh. The tape (e.g. Monarc) is positioned under the urethra and the incisions are the closed with stitches. These stitches will dissolve spontaneously. During the procedure, a telescope may also be passed through the urethra (water pipe) to examine the inside of the bladder (cystoscopy). The whole operation takes about 30 minutes.
In general, it is wise to try simple remedies as these may be successful and make surgery unlikely. Pelvic floor exercises can help in many cases. When taught by a physiotherapist, these can work very well. Like any exercise programme, it is necessary to keep doing them for them to work.
In addition, it is possible to try a drug called duloxetine. The trade name for this drug is "Yentreve". It needs to be taken twice a day indefinitely. It may be used in combination with physiotherapy. It is not as effective as a surgical procedure, needs to be taken twice a day and has side-effects. In some situations, it may be preferable in some cases.
Another operation was used in the past. This was called the Burch colposuspension and to many is still the gold standard by which all other procedures are judged. As it involves an incision made in the lower belly and requires several days in hospital, many people have chosen not to have this procedure because newer procedures require less time in hospital and are equal effective.
More recently, the TVT has been introduced as an innovative procedure for incontinence. The original TVT was placed behind a bone (pubis) in front of the bladder felt in the lower abdomen. As the approach required the passage of needles behind this bone, injuries that occurred from time to time to the bladder or bowel. The newer transobturator approach is much less likely to cause such problems and is preferable.
When you return to the ward, there may be a catheter present. This is a tube draining the bladder. If there is a catheter, this is usually removed after a few hours. If your bladder does not empty properly, it may be necessary to have a catheter for a longer period of time, but this is unusual. After you have passed urine, you can leave the ward and go home. This may be the same day, or sometimes the day after the operation. If the operation has been combined with a procedure for prolapse, you will probably be in hospital for a longer period of time.
You may need to take antibiotics for a while to prevent infection, and apply oestrogen cream (e.g. Vagifem tablets) to the vagina to promote healing.
The stitches present in the vagina and thigh dissolve spontaneously over a few weeks.
After 4 to 6 weeks, you should be reviewed by your doctor who may want to test the rate at which you pass urine and how effectively you empty your bladder. These tests are simple and are not invasive. After that you will probably be reviewed between 6 and 12 months after the operation.
Vesicovaginal fistula (VVF) is the most common acquired fistula of the urinary tract and has been known since ancient times. This is an abnormal communication between the urinary bladder and vagina leading to continuous leakage of urine.